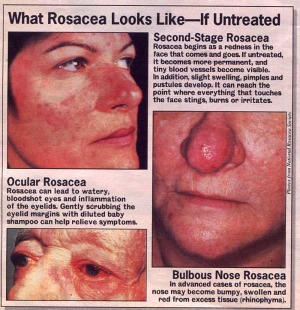
Ocular Rosacea
Have you noticed prominent, dilated blood vessels (known as telangiectatic vessels) on your cheeks? Does your nose look swollen and red? You may have Rosacea. Are your eyelids red and swollen? You may also have Ocular Rosacea.
What is Ocular Rosacea?
Ocular Rosacea is a subtype of a chronic skin condition called Rosacea.
Rosacea is marked by a range of signs and symptoms that include one or more primary features, usually found in the central area of the face:
Facial flushingFacial redness due to dilated blood vessels on the cheeksPapules and pustules that resemble acneRosacea has the following features:
Symptoms come and goMore common in fair-skinned individuals, but is probably under-reported in ethnic populations with darker skinPeak incidence occurs during the fourth to seventh decade of life Women are affected two to three times more often than menCondition often more severe in men Commonly affects the cheeks in women and the nose in men Rosacea can also affect the eyes. The incidence of eye findings in Rosacea based on varies studies is somewhere between 3% and 58%. In approximately 20% of Rosacea patients, ocular signs and symptoms are present before skin changesBased on a new classification system of Rosacea, eye findings were not only regarded as secondary features of the condition that could occur with primary skin findings, but also could appear independently. Ocular Rosacea is marked by a host of ocular signs.
What are signs and symptoms?
Ocular signs of Ocular Rosacea are a result of the inflammatory skin condition, specifically inflammation from Staphylococcus exotoxins.
Common signs due to the chronic ocular surface inflammation include:
 Meibomian gland plugging (that is, clogging of the oil glands of the lid margins)
Blepharitis
Meibomian gland plugging (that is, clogging of the oil glands of the lid margins)
Blepharitis
Dry eyes
Conjunctivitis
Recurrent
Chalazion
and HordeolumKeratitis
Ocular symptoms of Ocular Rosacea include:
 Eye drynessForeign-body sensationBurning and stingingTearingEye strain
Eye drynessForeign-body sensationBurning and stingingTearingEye strainCorneal involvement is the sight-threatening manifestation of Ocular Rosacea and can range from Superficial Punctate Keratitis, Marginal Corneal Infiltrates and
Corneal Ulcers
to Corneal clouding, Neovascularization, thinning and perforation.
What is the treatment?
The treatment of Ocular Rosacea is similar to that used for Rosacea. Naturally, treatment will depend on the type of Rosacea and the severity of the condition.
Tetracycline derivatives have been the central part of treatment, but according to current research, they seem to provide moderate benefit in the treatment of Ocular Rosacea.
The advantage of Tetracycline is that it decreases bacterial lipase, which improves the solubility of oil glands secretions.
Doxycycline is an effective tetracycline derivative. A typical dosing regimen is 100 mg doxycycline twice per day for six weeks, followed by once per day for two to four weeks.
Sometimes longer term therapy will be necessary to treat your Rosacea and a lower dose (such as 20 mg) form of doxycycline may be prescribed for you to take once or twice per day.
Tetracycline has its disadvantages as well. The drug is not recommended for children, pregnant women and nursing mothers. If you have poor kidney function, you should not take it.
Among its side effects are upset stomach, light sensitivity and even an eye condition marked by swelling of the Optic Nerve (as seen in a condition called Pseudotumor Cerebri). Erythromycin may be a viable alternative antibiotic.
Metronidazole is another medical therapy for Rosacea because of its antimicrobial, anti-inflammatory and immunosuppressive properties. You can take it orally or use it as a lotion. It is effective for inflammation but not for the chronically dilated vessels seen in the condition.
Topical steroids have been reported to be effective in the prevention of corneal erosions, which a sign of a more severe form of Ocular Rosacea.
However, the use of steroids in the eye can be associated with well-known side effects such as Cataract formation, thinning of the eyelid skin and elevated intraocular pressure.
A promising new drug for Ocular Rosacea may be azithromycin based on its positive results in the skin condition.
Azithromycin has few side-effects, limited drug interactions and good patient compliance. Its basic mechanism of action is believed to be by its anti-inflammatory properties.
For severe or recurrent Rosacea vitamin A derivatives such as Retinoids which suppress sebum production have been used.
Surgery as a mode of treatment has been gaining popularity in the field of Dermatology. A pulse-dye laser may be effective in reducing redness and dilated blood vessels in a type of Rosacea.
Other procedures like surgical ablation, electrocautery and carbon dioxide laser has been used to treat the rhinophyma (enlargement of oil glands of the nose).
How can you treat Ocular Rosacea?
Specific treatment for your Ocular Rosacea is going to involve managing the ocular signs and symptoms. Consult your eye care provider to get the best therapy.
First, you should treat any Blepharitis or Meibomianitis if either is present. Because the eyelids play an important role in producing and distributing the tear film, Blepharitis can affect vision by disrupting the surface of the cornea and the bulbar conjunctiva.
Implement simple therapies for mild signs of Dry Eyes such as lubricating tears. This may include the use of a humidifier at home or in the workplace.
If artificial tears alone are not giving you the relief you wish, the second level of defense is proper
nutrition
and
supplementation.
Omega-3 fatty acid supplementation has become a staple treatment for Dry Eyes. Omega-3 fatty acids have been shown to decrease inflammation, stimulate tear production and thin meibomian gland secretions.
Omega-3 fatty acids are available in eggs and fish like salmon. An excellent plant source of omega-3 fatty acids is flax seed. A recommended dose for supplementation is 1,000 mg to 2,000 mg per day.
Because inflammation is a problem with Rosacea, do not be surprised if your eye doctor recommends steroid
eye drops
for about 1.5 to 2 months. The steroid drop will be used four times per day for a month before being tapered.
If you experience significant relief from your dry eye symptoms with the steroid drops, then longer-term anti-inflammatory therapy will be used.
Since long-term use of steroids is not recommended because of potential side effects, Restasis (cyclosporine 0.05%), the only FDA-approved prescription medication for the treatment of Dry Eyes, will help combat inflammation long-term without the steroid potential side effects.
How else can you help?
Avoid trigger foods such as chocolate, tomatoes and citrus fruits, hot spices, alcohol and heated beverages. Avoid direct exposure to sunlight and always use appropriate amounts of sunscreen.
Seek help from a mental health provider if the changes in your facial appearance are causing anxiety, depression and poor self-esteem. You may just need some reassurance. Stress management may also be helpful.
Make sure you are seeing both your eye doctor and your dermatologist so that you are receiving the top level of treatment for all of your signs and symptoms.
Return From Ocular Rosacea to Eye Diseases
Enjoy this page? Please pay it forward. Here's how...
Would you prefer to share this page with others by linking to it?
- Click on the HTML link code below.
- Copy and paste it, adding a note of your own, into your blog, a Web page, forums, a blog comment,
your Facebook account, or anywhere that someone would find this page valuable.




