Amblyopia is the Condition of Decreased Central Vision
Have you been told that you have Amblyopia? Does that mean that your eyelid droops? Does it mean that your eye turns in or out?
Lazy eye is the condition of decreased central vision in an eye, usually since an early age in life. Lazy eye does not mean that your eyelid droops, a common misconception. Lazy eye can be caused by a variety of reasons:
Refractive Amblyopia or lazy eye can occur in one or both eye(s) and is characterized by high uncorrected refractive error. Refractive error can be high myopia (or nearsightedness), and/or irregular astigmatism. If this high refractive error is not corrected during the critical period of development (usually under age 6) in a child’s life, the proper neurological connections between the eye and the brain fail to be made.
This results in the brain “tuning out” the input of that particular eye, thus resulting in decreased vision. In the case of both eyes with high refractive error, the brain will “tune out” the input of both eyes, resulting in decreased vision in both eyes.
This decreased vision is not the result of any anatomical abnormality. The eye parts are where they should be and the eye is in good health. It is a higher level, neurological disconnect between the input of the optic nerve and the brain. It is not a macula problem.
Will your child never see better or will you never see well if you have Refractive Amblyopia?
The prognosis for good vision becomes guarded or poor, the older the person is when they get diagnosed. When Refractive Amblyopia occurs in only one eye and there is a large difference between the prescriptions of each eye, the management of the condition gets more complicated. When spectacles are prescribed with such disparate prescriptions, certain distortions occur optically and adaptation to glasses is difficult due to these uncomfortable effects.
Because early detection is critical to the successful management of Refractive Amblyopia, it is important to have your children’s eyes examined under the age of six by an optometrist or ophthalmologist. If Refractive Amblyopia exists only in one eye, it is easy to miss since a child can read well with both eyes open, or the child can peak under the cover of the good eye to read to letters on an eye chart.
Refractive Amblyopia is one of the few cases where wearing correction can actually help improve the vision. Because glasses can cause adaptation problems when the prescriptions between the eyes are very different, another excellent option is contact lenses.
Another important piece of managing this is to supplement the corrective devices (whether glasses or contact lenses) with vision therapy such as patching of the good eye in order to make the amblyopic eye work and practice seeing on its own.
Patching the good eye and using the amblyopic eye to do find-a-word, connect-the-dots, mazes, and other puzzles could be good vision therapy activities. Other treatment options include using atropine drops on the good eye to blur it so that the brain can rely more on the amblyopic eye.
What about if your eye turns in or out? Is that not also known as a lazy eye?
Yes, an eye turn, whether in or out, that is persistent can result in lazy eye, or amblyopia. This type of amblyopia is known as Strabismic Amblyopia. When an eye turns persistently in, or toward the nose, it is called Esotropia. When an eye turns persistently out, or toward the ear, it is called Exotropia.
If during the critical period of development, a child’s eye persistently turns in or out, then the child will suffer from diplopia, or double vision.
The brain does not like processing double images, and so will “tune out” the turned eye’s input. As a result, the child will have decreased vision in the turned eye. If this is not diagnosed early in the critical period of development, then the prognosis for treatment or management is guarded or poor.
What can be done for your eye turn? What can be done for your child’s eye turn?
If a persistent eye turn exists during the critical period of development, then it can be best managed with surgical intervention where the extraocular muscles are resected.
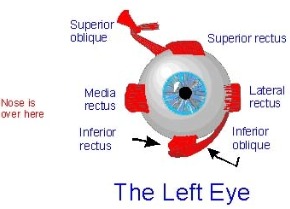
- Medial rectus moves the eye towards the nose
- Lateral rectus moves the eye away from the nose
- Inferior oblique rotates the eye so that the top of the eye moves away from the nose
- Superior rectus moves the eye up
- Superior oblique rotates the eye so that the top of the eye moves towards the nose
- Inferior rectus moves the eye down
In addition to surgery, patching therapy as described above should supplement the management. The patch would be placed over the good eye so that the turned eye can practice seeing. Of course any refractive error needs to be corrected for optimal vision with glasses or contact lenses.
If a persistent eye turn exists in an older patient, the prognosis for better vision in that eye is guarded or poor. Surgical intervention can be done, but it will be done more for cosmetic reasons than for functional reasons. Patching therapy can also supplement management. Here again, correcting refractive error is important.
What if your eyelid droops and covers the eye? Is that not a lazy eye?
If the eyelid droops as a result of age, trauma, or an acquired condition, this is not a lazy eye. This is referred to as ptosis. However, if a baby is born with an eyelid droop that covers the visual axis during the critical period of development, then this can result in lazy eye. This is referred to as Organic Amblyopia. Other causes of this are media opacities like congenital cataract and/or corneal opacities, or retinal diseases.
What is the treatment for Organic Amblyopia?
The treatment will involve treating the underlying condition, media opacity or retinal disease. If the cause is an eyelid droop, then surgical intervention to correct the droop is the management.
If the media opacity is a congenital cataract then surgical cataract extraction will be necessary and the baby can wear a special aphakic contact lens to correct their vision if an implant is not used. Underlying corneal diseases or retinal diseases need to be treated depending on the condition, but the prognosis for these conditions tends to be poor for good visual recovery.
What else should you know about?
Management involves treating underlying conditions, whether refractive error, eye turn, or anatomical abnormality such as eyelid droop, congenital cataract or congenital corneal or retinal disease. Correction of refractive error is important to maximize vision.
When glasses are ordered, the lenses should be ordered in polycarbonate material, which is a safety material. The reason for this is to protect the good eye from any damage since the person relies on it in the case of Amblyopia in one eye. Early detection and diagnosis is best in improving visual outcome.