




|
Eye Occlusion
Have you experienced sudden vision loss in one eye? Are you over the age of 50 (although younger patients are not immune)? Do you have other conditions like atherosclerosis, high cholesterol, diabetes, and hypertension (or high blood pressure)? You may have experienced an Eye Stroke or Eye Occlusion. What is an Eye Occlusion or Eye Stroke?
In order to view the content, you must install the Adobe Flash Player. Please click here to get started.
If you experience sudden vision loss you may be experiencing a Eye Occlusion or Eye Stroke. You need to go immediately to your eye care provider. Your eye doctor will check the location of the blockage and its extent. If you do have an Eye Occlusion or Eye Stroke you will have a blockage in either an artery or vein. The artery or vein involved will determine the extent of the damage. To function properly, brain cells need a constant supply of oxygen and glucose from the bloodstream. A Stroke is a disease that suddenly disrupts the brain’s function, usually by interfering with part of its essential blood supply and thus injuring brain cells. Like the brain, the eye has an essential blood supply which can be disrupted by an Eye Occlusion or Eye Stroke. Vital structures like the Retina or Optic Nerve can be cut off from the nutrients and oxygen flowing through your blood by an Eye Occlusion or Eye Stroke. The four main categories of an Eye Occlusion or Eye Stroke are listed below. Eye Occlusion: Central Retinal Artery Occlusion (CRAO)
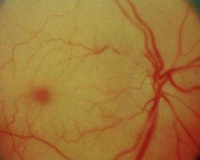
The cherry red spot in the left hand side of the photo is an eye occlusion. Central Retinal Artery Occlusion (CRAO) is an acute occlusion of the Central Retinal Artery (CRA). This means blood cannot flow into the Retina. This results in sudden, painless loss of vision in one eye. The Retina (which is normally transparent revealing the brownish-red color from the underlying Choroid) becomes whitish and opaque as the blood supply to the Retina is blocked. Another characteristic is “cherry-red spot”. The Retina overlying the Macula is relatively thin and the normal color of the Choroid is still visible in this area in contrast with the opaque Retina. This condition acts similarly to an Ischemic Cerebral Stroke (which is a stroke in the brain). If the artery remains blocked for more than a few minutes, the brain cells may die. Thus, immediate medical treatment is absolutely critical both in the case of brain strokes as in CRAO. Like in the Ischemic Cerebral Stroke situation, CRAO is caused by thrombi or emboli (blood clots). The blood clots can consist of cholesterol, calcified material, or platelet fibrin material. The goal of treatment is to give you a medication to break down the blood clot so that circulation can be re-established as soon as possible. Time is of the essence. Studies have shown that there is a time limit for CRAO to cause irreversible damage to the Retina. If retinal circulation is restored within this time limit, retinal function could recover. Other treatment options have been suggested to help restore circulation in a timely manner and help dislodge the blood clot. An example of an alternative method of treatment is to have Vitreous surgery (that is, remove the gel from inside the eye) and then massage the CRA in hopes of dislodging the clot and restoring circulation. Although no definitively effective treatment has been proven, any attempt is worthwhile since the prognosis is so grim if too much time elapses. Whatever the method used, the important point is to get timely care by seeing an ophthalmologist as soon as possible. Your next goal is to go to your general doctor and make sure that you don’t have any other health concerns or risk factors for CRAO: Branch Retinal Artery Occlusion (BRAO)

Branch Retinal Artery Occlusion (BRAO) has the same source of disease as CRAO; that is, an embolus (or blood clot). In the case of the BRAO, the embolus is small enough to pass through the parameter of the CRA. The embolus then moves into the retinal circulation, thus obstructing a branch of the CRA. The vision loss and the visual field loss are going to depend on the location of the blockage and the extent of blockage as well. At first, the affected arteries narrow and the retina becomes hazy. The retina will then whiten because of the lack of oxygen. The level of vision recovery is going to depend on timely treatment just like it does in the case of a CRAO. If there is more than a one to two hour delay in treatment, the chances of vision or visual field recovery is minimal. Also, like CRAO, the first priority is to attempt to reverse the occlusion and the next priority is to find out what may have caused it. Like CRAO, BRAO has a strong association with many of the same diseases listed above, especially internal carotid and heart disease. Eye Occlusion: Central Retinal Vein Occlusion (CRVO)
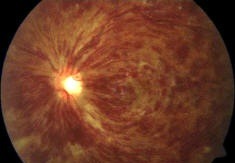
Central Retinal Vein Occlusion (CRVO) involves a blockage of the Central Retinal Vein (CRV). This means blood flow leaving the Retina is impeded causing a backup of blood in the eye resulting in leakage from capillaries, hemorrhage, retinal swelling, and Optic Nerve congestion. It typically occurs in people over the age of 50 and who have a systemic disease such as: Although Diabetes appears to have the least impact as a risk factor for CRVO, those patients who have Diabetes and experience CRVO tend to have more oxygen deprivation of their Retina than do non-diabetic patients. If you are younger than 50, you are less likely to have the diseases listed above, but you should be checked for blood clotting diseases. CRVO is a common, visually disabling eye disease affecting the Retina second in prevalence only to Diabetic Retinopathy. It usually occurs only in one eye. If it occurs in both eyes, you need to be checked for certain rare blood cancers. Symptoms of CRVO may include: In severe cases, the pupil in the affected eye will not work properly. Signs of CRVO include: The decrease of vision is mostly due to edema (or swelling) of the Macula. Another possible complication of CRVO, especially in the ischemic type (high oxygen deprivation), is neovascularization (or new blood vessel growth). Neovascularization is the way the body tries to supply the missing oxygen. These new blood vessels, however, are fragile and tend to bleed. Injections of a drug to help stop new blood vessel growth directly into the Vitreous have proven effective in reducing Macula Edema. This new blood vessel growth may occur in the iris (the colored part of the eye) and the anterior chamber of the eye, which may lead to a type of Glaucoma. More rarely, the new blood vessels may grow in the Retina or Optic Nerve. Managing CRVO thus will include looking out for these new blood vessels to grow and checking for Glaucoma. Unfortunately, as is the case with an Eye Occlusion or Eye Stroke, there is no proven effective treatment. For instance, steroid injections into the eye have been studied as a possible treatment, but eye pressure has to be monitored carefully since steroids can raise the eye pressure. Surgical options have been developed and studied to help CRVO as well. Eye Occlusion: Branch Retinal Vein Occlusion (BRVO)

Branch Retinal Vein Occlusion (BRVO) is more common than CRVO. The cause of BRVO may be any one of the following mechanisms or a combination of them: Symptoms of the condition: BRVO, like CRVO, are sorted into two categories: Over half of BRVO cases get better without treatment. However, BRVO rarely occurs without reason; rather it is frequently associated with other body problems like: The most important initial step in creating a management plan for this condition is to search for an underlying cause. In so doing, your doctor may require for you to have laboratory testing done, which may include the following: Check for other sources of Infection or Inflammation when other causes of BRVO are absent: Although a rare complication of BRVO, your eye doctor should check your eye pressure and your iris and anterior chamber for new blood vessel growth every four to six weeks for the first four months. The treatment for the Retina is aimed at controlling the Macula Edema and preventing new blood vessel growth. The standard of care for managing Macula Edema involves laser surgery (referred to as grid or focal photocoagulation) |